A recent article in the Health and Medicine section of The Conversation website:
https://theconversation.com/a-short-history-of-anaesthesia-from-unspeakable-agony-to-unlocking-consciousness-74748?utm_medium=email&utm_campaign=Latest from The Conversation for May 2 2017 - 72895553&utm_content=Latest from The Conversation for May 2 2017 - 72895553+CID_67e04e15f258af049914043ee1254fff&utm_source=campaign_monitor&utm_term=A short history of anaesthesia from unspeakable agony to unlocking consciousness
Author David Liley Professor, Centre for Human Psychopharmacology, Swinburne University of Technology
We expect to feel no pain during surgery or at least to have no memory of the procedure. But it wasn’t always so.
Until the discovery of general anaesthesia in the middle of the 19th century, surgery was performed only as a last and desperate resort. Conscious and without pain relief, it was beset with unimaginable terror, unspeakable agony and considerable risk.
Not surprisingly, few chose to write about their experience in case it reawakened suppressed memories of a necessary torture.
was by Fanny Burney, a popular English novelist, who on the morning of September 30, 1811 eventually submitted to having a mastectomy:
When the dreadful steel was plunged into the breast … I needed no injunctions not to restrain my cries. I began a scream that lasted unintermittently during the whole time of the incision … so excruciating was the agony … I then felt the Knife [rack]ling against the breast bone – scraping it.
But it wasn’t only the patient who suffered. Surgeons too had to endure considerable anxiety and distress.
John Abernethy, a surgeon at London’s St Bartholomew’s Hospital at the turn of the 19th century, described walking to the operating room as like “going to a hanging” and was sometimes known to shed tears and vomit after a particularly gruesome operation.
Discovery of anaesthesia
It was against this background that general anaesthesia was discovered.
A young US dentist named William Morton, spurred on by the business opportunities afforded by technical advances in artificial teeth, doggedly searched for a surefire way to relieve pain and boost dental profits.
His efforts were soon rewarded. He discovered when he or small animals inhaled sulfuric ether (now known as ethyl ether or simply ether) they passed out and became unresponsive.
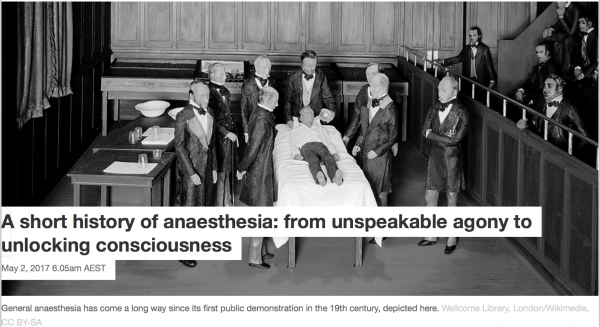
A few months after this discovery, on October 16, 1846 and with much showmanship, Morton anaesthetised a young male patient in a public demonstration at Massachusetts General Hospital.
The hospital’s chief surgeon then removed a tumour on the left side of the jaw. This occurred without the patient apparently moving or complaining, much to the surgeon’s and audience’s great surprise.
So began the story of general anaesthesia, which for good reason is now widely regarded as one of the greatest discoveries of all time.
Anaesthesia used routinely
News of ether’s remarkable properties spread rapidly across the Atlantic to Britain, ultimately stimu- lating the discovery of chloroform, a volatile general anaesthetic.
According to its discoverer, James Simpson, it had none of ether’s “inconveniences and objections” – a pungent odour, irritation of throat and nasal passages and a perplexing initial phase of physical agitation instead of the more desirable suppression of all behaviour.
Chloroform subsequently became the most commonly used general anaesthetic in British surgical and dental anaesthetic practice, mainly due to the founding father of scientific anaesthesia John Snow, but remained non-essential to the practice of most doctors.
This changed after Snow gave Queen Victoria chloroform during the birth of her eighth child, Prince Leopold. The publicity that followed made anaesthesia more acceptable and demand increased, whether during childbirth or for other reasons.
By the end of the 19th century, anaesthesia was commonplace, arguably becoming the first example in which medical practice was backed by emerging scientific developments.
Anaesthesia is safe
Today, sulfuric ether and chloroform have been replaced by much safer and more effective agents such as sevoflurane and isoflurane.
Ether was highly flammable so could not be used with electrocautery (which involves an electrical current being passed through a probe to stem blood flow or cut tissue) or when monitoring patients electronically. And chloroform was associated with an unacceptably high rate of deaths, mainly due to cardiac arrest (when the heart stops beating).
The practice of general anaesthesia has now evolved to the point that it is among the safest of all major routine medical procedures. For around 300,000 fit and healthy people having elective medical procedures, one person dies due to anaesthesia.
Despite the increasing clinical effectiveness with which anaesthesia has been administered for over the past 170 years, and its scientific and technical foundations, we still have only the vaguest idea about how anaesthetics produce a state of unconsciousness.
Anaesthesia remains a mystery
General anaesthesia needs patients to be immobile, pain free and unconscious. Of these, unconsciousness is the most difficult to define and measure.
For example, not responding to, or then not remembering, some event (such as the voice of the anaesthetist or the moment of surgical incision), while clinically useful, is not enough to decisively determine whether someone is or was unconscious.
This chloroform inhaler was the type John Snow used on Queen Victoria to ease the pain of childbirth. Chloroform vapours were delivered down a tube via the brass and velvet face mask. Science Museum, London/Wellcome Images/Wikimedia, CC BY-SA
We need some other way to define consciousness and to understand its disruption by the biological actions of general anaesthetics.
Early in the 20th century, we thought anaesthetics worked by dissolving into the fatty parts of the outside of brain cells (the cell membrane) and interfering with the way they worked.
But we now know anaesthetics directly affect the behaviour of a wide variety of proteins necessary to support the activity of neurones (nerve cells) and their coordinated behaviour.
For this reason the only way to develop an integrated understanding of the effects of these multiple, and individually insufficient, neuronal protein targets is by developing testable, mathematically formulated theories.
These theories need to not only describe how consciousness emerges from brain activity but to also explain how this brain activity is affected by the multiple targets of anaesthetic action.
Despite the tremendous advances in the science of anaesthesia, after almost 200 years we are still waiting for such a theory.
Until then we are still looking for the missing link between the physical substance of our brain and the subjective content of our minds.